The primary objective of apreparation is to preserve as much sound structure as possible while reinforcing weakened areas, increasing the adhesive surface area, and ensuring the long-term functional success of the restoration. Before the preparation, the vitality of the tooth, the extent of structural loss, the presence of existing restorations, occlusal load distribution, and the relationship with the antagonist dentition should be carefully evaluated. All carious tissues and existing restorations must be removed, and the preparation should be completed until healthy tooth structure is reached.
For layered composite restorations, a minimum occlusal reduction of 2 mm is recommended. In monolithic restorations (e.g., lithium disilicate or ceramic-reinforced resin-based materials), a reduction of 1.0–1.5 mm is generally considered safe to prevent material fracture and clinical complications.
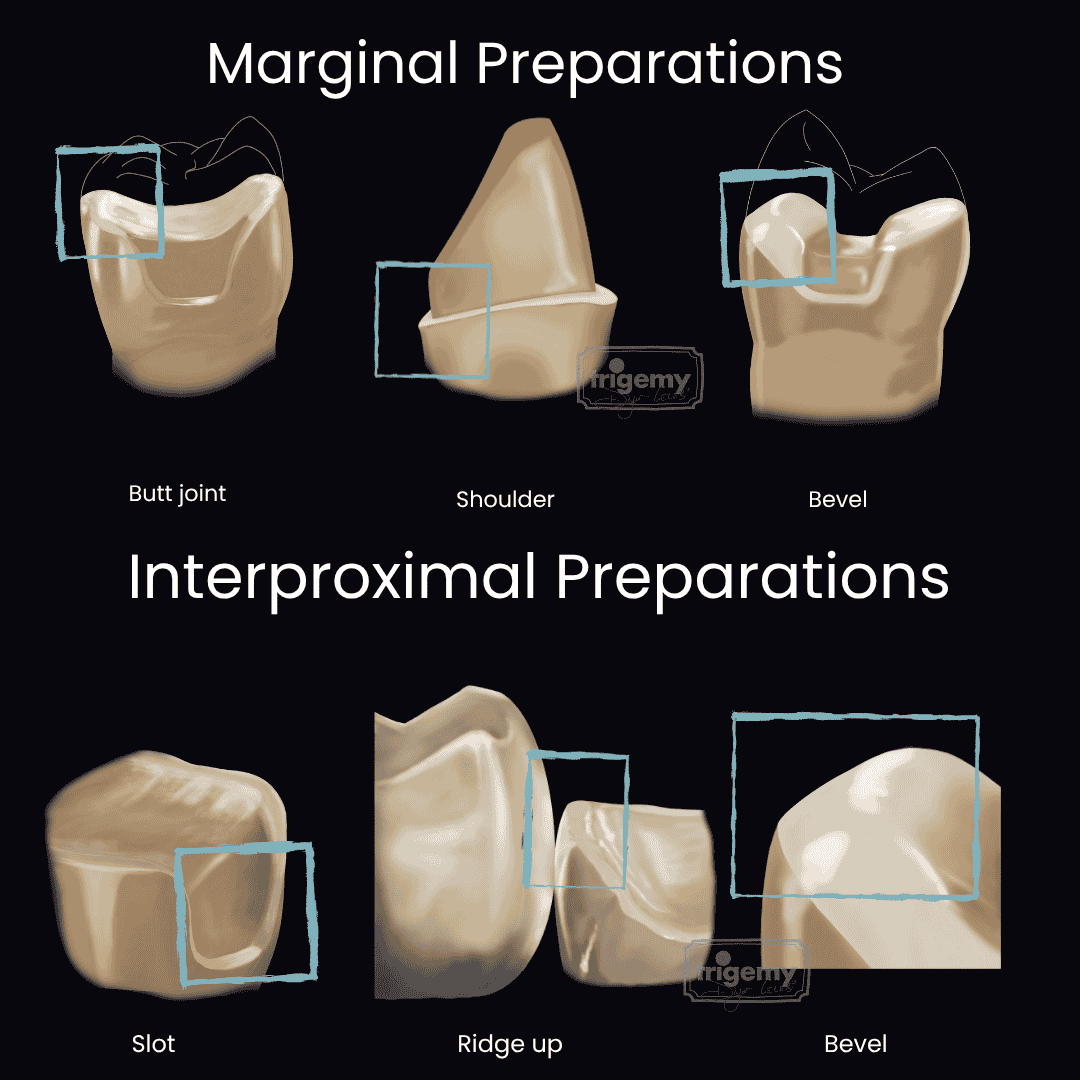
Butt joint: 90° flat margin; provides the highest strength and adaptation.
Shoulder: A flat margin approximately 1 mm in width; preferred in areas requiring increased material thickness.
Bevel: An inclined margin; increases enamel surface area and improves esthetic transition.
Cusp thickness should be ≥2 mm in vital teeth and ≥3 mm in non-vital teeth. If these values are not met, cusp coverage is recommended. This approach helps transfer occlusal forces to dentin support, thereby reducing the risk of fracture. The central isthmus width should be maintained at ≥2 mm. Internal line angles must be rounded, and sharp edges should be avoided. Transitions from the occlusal surface to axial walls should be smooth and continuous. Axial walls should be prepared with slight divergence.
Slot: Approximately 1 mm wide with a rounded shoulder form. It is commonly formed during the removal of interproximal caries and is therefore frequently preferred in posterior regions. This design allows adequate structural support for the restoration.
Bevel: More conservative than the slot preparation and prevents unnecessary cervical extension. It increases enamel surface area, thereby enhancing adhesive cementation. It is indicated when no caries is present, when a wide interproximal restoration is required, and when the contact point is located more cervically.
Ridge up: Compared to bevel preparation, it preserves the integrity of the marginal ridge. Even when the marginal ridge is included, it maintains the contact area with minimal surface preparation. The marginal ridge is one of the most critical structures for maintaining the integrity of non-vital teeth. Therefore, if adjacent cusps are weakened, cusp coverage may be preferred while preserving the marginal ridge. This design is indicated in cases where structural preservation is essential, the marginal ridge is intact, and no cavitated carious lesions are present.
Immediate Dentin Sealing (IDS) is particularly indicated when a large dentin surface is exposed. It protects the dentin from bacterial, environmental, and thermal effects between impression and cementation, while also enhancing adhesion.
After IDS, any undercut areas should be blocked out using flowable composite. If the margin is located below the gingival level, deep margin elevation should be performed to relocate the margin coronally.
At the end of the preparation, all surfaces should be smoothed using fine-grit diamond burs.
Ferraris F. Posterior indirect adhesive restorations (PIAR): Preparation designs and adhesive clinical protocol. Int J Esthet Dent. 2017;12(4):482–502.
We use cookies to ensure the best experience on our website. By continuing to browse this site, you agree to our use of cookies. Learn more in our User Agreement, Privacy Policy, and GDPR Notice.